
History
Trigger finger was first described in 1850 by Alphonse Notta, during his internship at I’hôpital Saint-Louis. His patient was a seamstress, he wrote “When all the fingers of the right hand are flexed and the patient wants to straighten them, all the fingers straighten out comfortably except the middle finger which begins to straighten then it stops. The patient then forcefully straightens out her extensors, a brisk movement occurs.” In other words her finger gets stuck and then opens with a pop. “ Very often this extra

effort of the extensors is not enough and her finger remains flexed. The patient then uses the extremity of the right thumb and lifts the last phalanges of the middle finger a little, this then allows her finger to be extended”1. In other words sometimes its so bad she must use the other finger to open her affected finger.
Notta, published his observation in 1850 stating that, “the medical condition described in these case studies pertains to a nodosity on the span of the flexor tendons of some fingers. This nodosity encounters obstacles when fingers are being bent and stretched... What is the cause of this nodosity? What obstacles does it encounter?’’1.
Who gets trigger finger?
The life time risk of developing a trigger finger is 2-3% and it occurs six times more frequently in women in their fifth and sixth decades of life. It can happen to all fingers but the ring finger and the thumb are the most frequently affected. The risk is increased to as much as 10% among people with diabetes mellitus.
After 167 years there is still no clear consensus in the scientific literature about what causes trigger finger. However, even Notta knew that often times it can be work related as he noted “repetitive occupational micro trauma to the tendon” from her constant sewing1. However, the majority of cases idiopathic nature, which simply means we don’t know what causes it.
There are common association however, such as the pre-existence of other diseases like carpal tunnel syndrome, diabetes, rheumatoid arthritis, gout, and amyloidosis.
How does it happen?
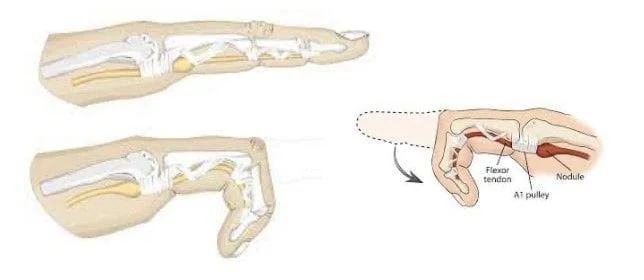
Under normal circumstances, the flexor tendons must glide quietly through the pulley system during flexion and extension of the digits. The pulley system can be thought of as a series of D-Rings on the palmar surface of the finger.
During forceful finger flexion or power grip, there is considerable angulation of the tendons at the proximal edge of the A1 pulley. This acts as a fulcrum or the constricting element which can cause pain. In early stages this will cause a pain in the palm without “clicking”. In later stages this will cause an inflammatory nodule in the tendon. The nodule must squeeze through the pulley.
What kind of symptoms do patients describe?
Patients often describe hand pain that is worse when they wake up and, becomes less bothersome as the day progresses. Trigger finger is graded based on four levels of severity.
Grade 1 A patient may present with a slight discomfort or tenderness in the involved digit localized to the base of the finger. There maybe minimal or no history of catching.
Grade 2 A patient may feel a mild click in the finger or may report difficulty extending the finger. At this stage however if the patient tries he/she/they are able to extend with their own power.
Grade 3 The patient will be unable to to fully flex the finger or extend it without the help of the other hand. With progression of the disease, there is distinct discomfort on the palmar side of the knuckle joint, with pain frequently radiating into the forearm. When triggering occurs, the patient will often feel a snapping as occur at the first finger joint.
Grade 4 The finger catches and is no longer able to open.
What are the treatment options?
Injections
The first line treatment for trigger finger is an injection of locally
acting corticosteroids. There are various studies that demonstrate cure
rates from 30% - 90%. In my experience the vast majority of patients
presenting with trigger finger will be cured with either one or two
injections.
Surgery
After a trial of steroids if the trigger finger symptoms persist the
definitive cure is surgery. The surgery can be done in a minimally invasive
fashion under the guidance of ultrasound or in a standard open fashion.
While either approach is exceedingly safe Each approach has its own sets of
risks and benefits which are best discussed in detail in person.